Survodutide vs. Retatrutide vs. Tirzepatide: A Comparative Research Review
1.The Post-Ozempic Era
For nearly a decade, the landscape of metabolic research was dominated by a single molecule: Semaglutide. As a mono-agonist targeting the Glucagon-like peptide-1 (GLP-1) receptor, it revolutionized the treatment of Type 2 Diabetes and obesity. However, in the fast-moving world of peptide development, the era of the mono-agonist is already fading.
We have entered the age of poly-agonism—molecules designed to hit multiple biological targets simultaneously. By recruiting additional hormonal pathways, researchers are unlocking synergy that was previously thought impossible: weight loss approaching bariatric surgery levels, profound liver fat reduction, and complete remission of metabolic syndrome markers.
Currently, three giants stand at the forefront of this revolution:
-
Tirzepatide (Mounjaro/Zepbound): The reigning champion, a dual GLP-1/GIP agonist that broke the “20% weight loss” barrier.
-
Retatrutide (LY3437943): The challenger, a “triple agonist” (GLP-1/GIP/Glucagon) that promises even greater potency.
-
Survodutide (BI 456906): The specialist, a dual GLP-1/Glucagon agonist that ditches GIP entirely in favor of a potent liver-targeting mechanism.
For researchers in the UK, the question is no longer “do incretins work?” but rather “which agonist profile is superior for my specific endpoint?” Is the triple action of Retatrutide necessary for everyone? Does Survodutide’s unique “glucagon backbone” offer advantages for non-alcoholic steatohepatitis (NASH) that Tirzepatide cannot match?
This comparative review details the Battle of the Agonists. We will dissect the molecular mechanisms, analyze the Phase 2 and Phase 3 efficacy data, and scrutinize the side effect profiles to provide a definitive technical guide for the research community.
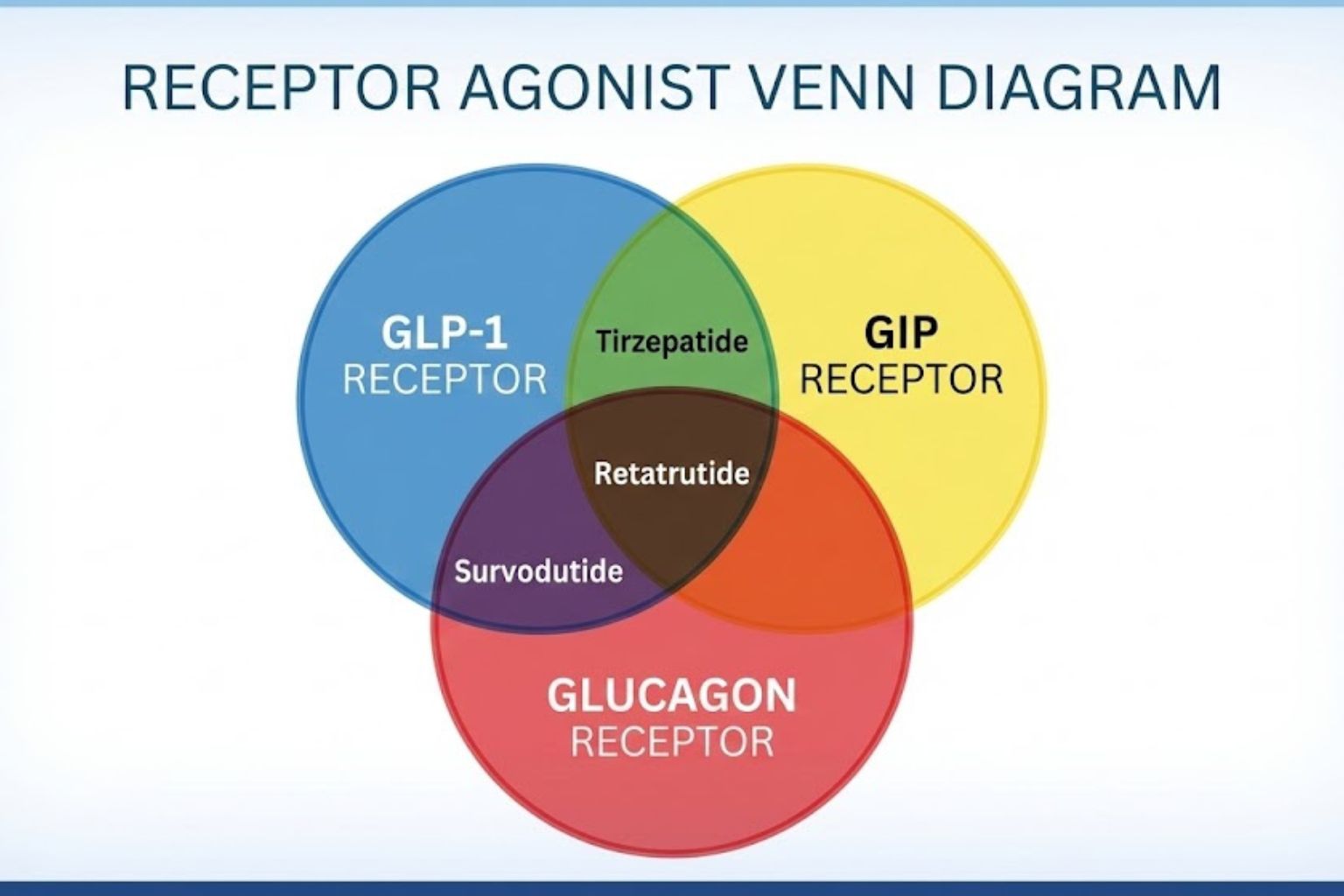
2. Mechanism Breakdown: The Receptor Wars
To understand the difference between Survodutide vs Retatrutide, one must first understand the receptors they target. These peptides are not merely stronger versions of one another; they are chemically distinct tools that manipulate human physiology in different ways.
Tirzepatide: The “Twincretin” (GLP-1 + GIP)
-
The Targets: Glucagon-like peptide-1 (GLP-1) and Glucose-dependent insulinotropic polypeptide (GIP).
-
The Strategy: Tirzepatide was the first to successfully leverage the “incretin effect” of GIP. Historically, GIP was thought to be “obesogenic” (promoting fat storage). However, Tirzepatide proved that when combined with GLP-1, GIP actually enhances insulin secretion and acts centrally in the brain to reduce nausea, allowing for higher dosing of the GLP-1 component.
-
Receptor Activity: It is imbalanced by design, favoring the GIP receptor over the GLP-1 receptor. This unique ratio is key to its tolerability.
Retatrutide: The “Triple G” (GLP-1 + GIP + Glucagon)
-
The Targets: GLP-1, GIP, and Glucagon (GCG).
-
The Strategy: Retatrutide takes the Tirzepatide scaffold and adds a third weapon: Glucagon.
-
Why Glucagon? In isolation, Glucagon raises blood sugar (which is bad for diabetes). However, it also powerfully increases Energy Expenditure (EE) by stimulating brown adipose tissue and increasing mitochondrial oxidation. By balancing Glucagon with GLP-1 (which lowers blood sugar), Retatrutide aims to “burn” calories while “suppressing” appetite. It is the metabolic equivalent of hitting the brake (appetite) and the gas (metabolism) simultaneously.
Survodutide: The “Liver Specialist” (GLP-1 + Glucagon)
-
The Targets: GLP-1 and Glucagon. (No GIP).
-
The Strategy: Survodutide is distinct because it ignores the GIP pathway entirely. Instead, it focuses on a direct symbiotic relationship between GLP-1 and Glucagon.
-
The Glucagon Backbone: Unlike Tirzepatide (which is based on a GIP backbone), Survodutide is chemically derived from the native Glucagon sequence. This gives it a unique affinity for the liver.
-
The Ratio: It is highly biased towards GLP-1 (activity ratio approx 8:1). This is a safety mechanism. The GLP-1 effect must overpower the Glucagon effect to ensure blood glucose doesn’t spike. The Glucagon activity is kept “sub-maximal”—just enough to stimulate lipolysis (fat breakdown) in the liver and reduce body weight, but not enough to cause hyperglycemia.
3. Efficacy Data: The Race for Weight Loss
When comparing Survodutide vs Retatrutide in terms of raw weight loss, the data from Phase 2 trials paints a clear hierarchy. However, “more” is not always “better” for every context.
Tirzepatide (The Benchmark)
-
Study: SURMOUNT-1 (Phase 3).
-
Results: At 72 weeks, the highest dose (15mg) achieved a mean weight loss of 20.9%.
-
The Ceiling: Tirzepatide set the new standard, proving that pharmaceutical weight loss could exceed the 15% barrier previously thought to be the limit for non-surgical interventions.
Retatrutide (The Heavyweight Champion)
-
Study: Phase 2 Trial (published in NEJM).
-
Results: At 48 weeks, the highest dose (12mg) achieved a mean weight loss of 24.2%.
-
Projection: Notably, the weight loss curve for Retatrutide had not plateaued at 48 weeks. Models suggest it could approach 28-30% at 72 weeks, rivaling the efficacy of gastric bypass surgery.
-
The Triple Advantage: The addition of Glucagon-mediated energy expenditure appears to strip fat faster than appetite suppression alone.
Survodutide (The Contender)
-
Study: Phase 2 Dose-Finding Study.
-
Results: At 46 weeks, the highest tested dose (4.8mg) achieved a mean weight loss of 14.9% (treatment policy estimand) to 18.7% (trial product estimand).
-
The Comparison: On paper, Survodutide appears “weaker” than Retatrutide for pure scale weight reduction. It falls closer to the efficacy of Semaglutide 2.4mg (Wegovy) or lower-dose Tirzepatide.
-
Nuance: However, Survodutide’s trials often focus heavily on specific populations (like NASH patients), where the primary goal is organ health, not just BMI reduction.
4. The “Glucagon Backbone” Difference: Why Survodutide Stands Apart
If Retatrutide causes more weight loss, why would a researcher choose Survodutide? The answer lies in the Glucagon Backbone and the absence of GIP.
Direct Liver Targeting
Survodutide is designed with a specific mission: Lipolysis. The Glucagon receptor is highly expressed in the liver. By agonizing this receptor, Survodutide drives the breakdown of triglycerides and fatty acids within the hepatocyte (liver cell).
-
Tirzepatide: Reduces liver fat indirectly by causing the patient to lose total body weight.
-
Survodutide: Reduces liver fat directly via chemical signaling, in addition to weight loss. Phase 2 data showed up to 83% of MASH (Metabolic dysfunction-associated steatohepatitis) patients achieved significant histological improvement.
The GIP Question
Some researchers hypothesize that GIP, being an insulinotropic hormone, might “protect” adipose tissue in some contexts or lead to different fat partitioning. By omitting GIP, Survodutide offers a “pure catabolic” approach. This makes it an invaluable research tool for separating the effects of GIP from the effects of Glucagon.
5. Side Effect Profile: The Cost of Agonism
Potency comes with a price. In the comparison of Survodutide vs Retatrutide, the side effect profiles reveal the physiological stress of activating multiple receptors.
Gastrointestinal (The Universal Tax)
All three peptides (Tirzepatide, Retatrutide, Survodutide) cause the classic “GLP-1 GI Triad”: Nausea, Diarrhea, and Vomiting.
-
Tirzepatide: Generally well-tolerated due to the anti-emetic properties of GIP.
-
Retatrutide: Phase 2 data showed higher rates of nausea compared to Tirzepatide, likely due to the triple potency.
-
Survodutide: Dose-escalation must be very slow. The Glucagon component can relax smooth muscle in the gut, potentially compounding the gastric slowing of GLP-1.
Heart Rate (The Glucagon Tax)
This is the most critical safety differentiator. Glucagon receptors are present in the heart (sinoatrial node). Activating them can increase heart rate (chronotropy).
-
Tirzepatide: Causes a mild increase in resting heart rate (1-4 bpm), typical of GLP-1s.
-
Survodutide & Retatrutide: Both have shown more pronounced increases in heart rate in Phase 2 trials, sometimes peaking at +5 to +10 bpm.
-
Arrhythmia Risk: Researchers monitoring these peptides must be vigilant for arrhythmias. The “Glucagon tax” is increased cardiac workload. For young, obese patients, this is negligible. For elderly patients with existing cardiovascular disease, it is a significant research variable.
Cutaneous Sensitivity
Interestingly, Retatrutide trials noted a higher incidence of “cutaneous hyperesthesia” (skin sensitivity/tenderness) compared to other incretins. The mechanism is unknown but may be linked to GIP/Glucagon interactions in peripheral nerves.
6. Research Applications: Selecting the Right Peptide
For the UK researcher designing a study, which peptide should you choose?
Scenario A: Maximum Obesity Reversal
-
Choice: Retatrutide.
-
Rationale: If the goal is to test the absolute limits of pharmacological weight loss—perhaps comparing drug therapy to bariatric surgery—Retatrutide is the only candidate with the potency to win that fight.
Scenario B: Liver Fibrosis & NASH/MASH
-
Choice: Survodutide.
-
Rationale: Survodutide is effectively a “liver drug that causes weight loss.” Its data on fibrosis reduction is class-leading. If your research model involves hepatic steatosis, fibrosis markers, or liver enzyme kinetics, Survodutide is the most mechanistically interesting candidate.
Scenario C: Diabetes Management with Tolerability
-
Choice: Tirzepatide.
-
Rationale: It is the proven entity. With FDA/MHRA approval and years of safety data, it represents the “Gold Standard” control arm. It balances profound glucose control (better than Survodutide) with excellent weight loss.
7. Future Outlook: The Timeline
-
Tirzepatide: Available now (Research & Clinical). The focus is now on new indications (Sleep Apnea, Kidney Disease).
-
Survodutide: Currently in Phase 3 trials (SYNCHRONIZE program). Results expected late 2025/2026. Boehringer Ingelheim is positioning it aggressively for MASH.
-
Retatrutide: Currently in Phase 3 trials (TRIUMPH program). Results expected 2026. Eli Lilly is positioning it as the ultimate obesity solver.
8. Comparative Summary Table
9. The Right Tool for the Right Biological Question
The “Battle of the Agonists” is not a zero-sum game. Retatrutide is not simply “better” than Survodutide because it induces more weight loss.
-
Retatrutide proves that targeting energy expenditure (via Glucagon) alongside appetite (GLP-1/GIP) is the key to breaking metabolic adaptation.
-
Survodutide proves that you don’t need GIP to fix a fatty liver, and that a targeted Glucagon/GLP-1 approach may be the holy grail for hepatology.
For the peptide researcher, these molecules represent a toolkit of unprecedented precision. By understanding the distinct mechanism of the Survodutide vs Retatrutide comparison, you can design experiments that are not just checking for weight loss, but probing the very nature of human metabolism.
10. References
-
Jastreboff, A. M., et al. (2023). Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. New England Journal of Medicine.
-
Rosenstock, J., et al. (2021). Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1). The Lancet.
-
Le Roux, C. W., et al. (2023). A Phase 2, Randomized, Double-Blind, Placebo-Controlled, Dose-Finding Trial of Survodutide (BI 456906) in People With Overweight or Obesity. Annual Meeting of the European Association for the Study of Diabetes.
-
Finan, B., et al. (2015). A rationally designed monomeric peptide triagonist corrects obesity and diabetes in rodents. Nature Medicine.